
The District of Columbia Fire and Emergency Medical Services (DC FEMS) embodies a sophisticated approach to emergency management, integrating fire rescue and emergency medical services through a seamless operational system. This article provides a thorough examination of DC FEMS’s key operational features and how they effectively respond to various emergencies within the district. From the innovative integrated response model that ensures rapid and effective medical care at the scene, to specialized units that handle unique emergencies, we explore crucial facets of their operations. Additionally, we will highlight the role of public education and preventative measures in emergency preparedness. By illuminating these aspects, readers will appreciate the essential work of DC FEMS and how it enhances community safety and resilience.
Integrated Response at the Nation’s Capital: How DC FEMS Orchestrates Fire, EMS, and Law Enforcement for Rapid Life-Saving Action
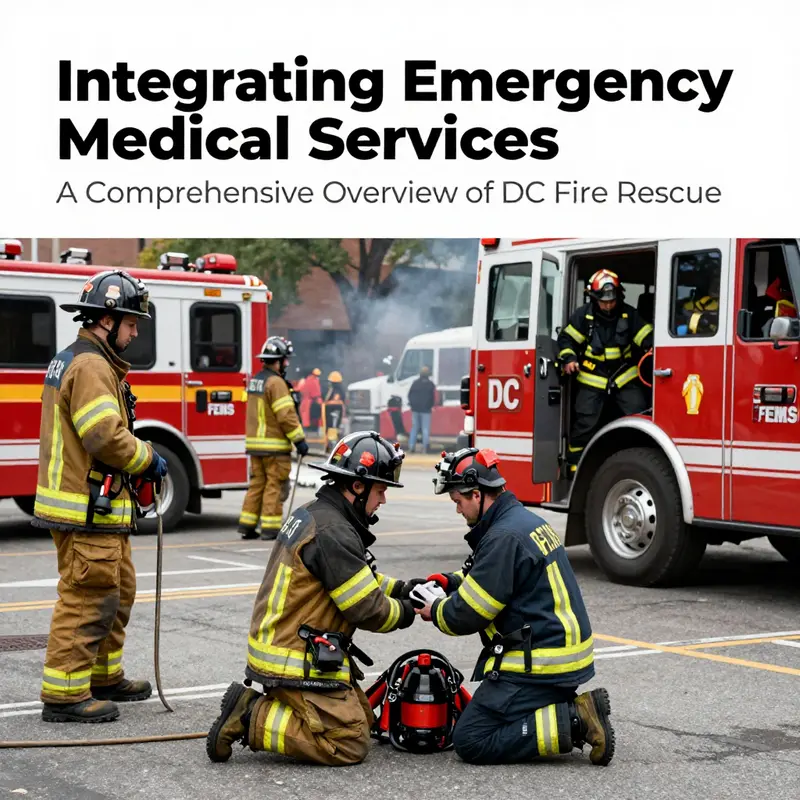
In the District of Columbia, the line between firefighting and emergency medical care is purposefully blurred, not blurred by accident but by design. DC FEMS operates as a single, cohesive emergency response system where fire suppression, advanced medical care, hazardous materials response, technical rescue, and public education all flow from one organizational core. This integrated approach marks a departure from models that treat fire suppression and EMS as separate silos. The momentum behind this design rests on a simple, high-stakes premise: life-saving care should begin at the moment responders arrive on scene, not after a patient is loaded into a separate ambulance. To achieve that end, every firefighter in the DC system is trained as an emergency medical provider, capable of delivering advanced life support as soon as a crew arrives. This means that when a call comes in, the first units on scene are not just engines standing by for water or access—they are teams of clinicians who can perform airway management, monitor cardiac rhythms, administer critical medications, and initiate treatment for trauma or medical emergencies before a patient ever boards an ambulance. The result is a marked reduction in the delay between incident onset and the patient receiving advanced care, which is especially consequential in time-critical conditions such as cardiac arrest, stroke, or severe trauma.
If the status quo could be imagined, it would feature engines that look and feel like mobile ICUs, staffed by personnel who blend the disciplines of firefighting and emergency medicine. DC FEMS makes that vision a daily reality through an integrated response model that has several defining elements. First, rapid response times are not aspirational goals but operational imperatives. Citywide, the average response time for medical emergencies remains within a five-minute window, a pace that keeps the system focused on outcomes rather than logistics alone. This speed is achieved not only by the proximity of units but by the operational discipline that common training and shared protocols provide. Second, specialized units exist to anticipate and handle the outliers—the HazMat teams to address chemical threats, technical rescue units for complex entrapments or high-angle rescues, and the Mobile Intensive Care Unit (MICU) to transport critically ill patients with the full array of life-support capabilities already in motion. These elements do not function in isolation; they operate within a unified framework where command, control, and medical care are coordinated from the earliest moments of a response. Public education and prevention, including CPR/AED training and home safety inspections, reinforce this operational posture by reducing risk and building community resilience before emergencies arise. The results of this integrated philosophy extend beyond individual calls to shape a culture of preparedness and rapid, coordinated action across all districts in the capital.
A cornerstone of the DC FEMS Integrated Response Model is its formal incorporation of law enforcement into the same command architecture used by fire and EMS responders. This is not a matter of parallel, adjacent responses but a true integration that recognizes the realities of many urban emergencies, where scene security, crowd control, and medical care must be negotiated in real time. The Integrated LEO-EMS Rescue Task Forces (RTFs) epitomize this approach. RTFs are specially trained teams that bring together law enforcement, fire, and EMS personnel to respond jointly to high-risk events such as active shooter scenarios or mass casualty incidents. The protocols governing RTFs are aligned with national frameworks like the National Incident Management System (NIMS) and the Hospital Incident Command System (HICS), ensuring that everyone speaks a common language during chaos. The unified command structure that underpins these efforts replaces duplicate radio chatter with a clear, shared picture of the incident. In practice, this means that decision-making is not devolved through a chain of separate agencies but is centralized in a single, coordinated command, with rapid information sharing powering that coordination.
The strength of a unified approach shows up most clearly in real-time information sharing. When a call lands, responders don’t trade silos for silos; they trade information—maps, capabilities, patient statuses, and evolving threat assessments—so that every decision is grounded in a common understanding. In a complex incident, this shared situational awareness can be the difference between timely life-saving care and missed opportunities. The 2025 evaluation of the integrated LEO-EMS Rescue Task Force model in a large urban setting highlighted several measurable improvements: faster response times, clearer communication, and stronger on-scene decision-making. In simulations involving active shooter and mass casualty scenarios, the shared command structure consistently produced better outcomes than operations conducted by separate, uncoordinated teams. These findings, while derived from drills, reflect the real-world potential of the DC FEMS model when deployed under the stress of actual events.
The Integrated Response Model is more than a procedural rearrangement; it is a blueprint for deploying resources where they are most likely to save lives. Rapid deployment becomes feasible because assets are designed to operate in concert from the outset. Mutual aid, a staple of urban emergency response, is streamlined by pre-agreed protocols and standardized equipment that can be deployed without lengthy negotiations or last-minute lead times. This is not simply about faster fire suppression or quicker EMS transport; it is about ensuring that the handoffs between tactical and medical operations are seamless. When HazMat teams, technical rescue units, MICUs, and regular engine companies converge at a complex scene, they do so with a shared mental model, a common lexicon, and a direct, uncluttered channel of communication. The integrated approach reduces the friction that can occur when different agencies interpret the situation through separate lenses, leading to delays, duplicated efforts, or conflicting priorities. In DC, the integration is designed to protect life at the scene and to preserve the potential for a favorable hospital outcome by ensuring that transport decisions and on-scene care are guided by a single strategic objective.
Training and preparation sit at the heart of this model. The authoritative DC FEMS NAEMT collaboration document outlines rigorous training protocols, standardized equipment, and joint exercise requirements that bind fire, EMS, and law enforcement into a cohesive unit. The emphasis is on practical, drills-based learning that mirrors the realities responders face in the urban environment. What emerges from this approach is not a rigid script but a flexible, resilient system capable of adapting to the unpredictable nature of emergencies. A shared training culture translates into a shared sense of purpose: to minimize the time to definitive care and to maximize the probability of positive outcomes for patients and communities alike. The public-facing aspects of this model—community CPR training, safety education, and prevention programs—are not afterthoughts but integral elements that sustain the cycle of readiness and response. By educating the public, DC FEMS reduces the number of high-acuity calls and empowers residents to act decisively in the crucial minutes before responders arrive.
This integrated ethos, however, does not negate the need for specialized constructs within DC FEMS. The MICU represents a pinnacle of medical capability within the field response framework. It is equipped to handle the transport of critically ill patients, ensuring that advanced therapies remain available en route to the hospital. HazMat teams provide the specialized knowledge and equipment required to manage chemical or toxic hazards, protecting responders and the public while enabling medical teams to deliver targeted interventions. Technical rescue units address the most demanding extraction and stabilization tasks—scenarios that demand precision, calm under pressure, and a careful balance between speed and safety. When these units operate under the Unified Command, they contribute to a coherent, life-saving continuum from the moment a call is received to the point where the patient is handed off to hospital care.
The practical implications of this model extend beyond the emergency scene. DC FEMS’s integrated approach has a ripple effect that touches every layer of the city’s public safety and health landscape. By flattening the response timeline and aligning medical care with tactical operations, DC reduces the likelihood of deterioration in the minutes after an incident, raising the probability of survivability and favorable neurological outcomes. The model also supports mutual aid dynamics, allowing neighboring jurisdictions to participate in a manner that preserves the integrity of the incident command and the quality of care provided to the patient. In short, the Integrated Response Model is a system-wide philosophy that treats the first five minutes of any emergency as a critical window in which decisive action, clear communication, and a unified command can change the trajectory of an event.
For readers seeking a deeper dive into the official architecture of this approach, DC FEMS and the NAEMT collaboration provide a comprehensive reference. The detailed report, including training, equipment standards, and joint exercise requirements, offers the practical blueprint behind the narrative of rapid integration in the nation’s capital. Innovation Museum: Transforming Fire Services provides a broader context for how innovations in training, technology, and cross-agency collaboration are reshaping the culture of readiness in urban emergency response. This broader framing helps connect the DC experience to a national conversation about integrated emergency services and the evolving role of firefighters as medical responders from the outset of every call. For a formal account and the most authoritative specifics, consult the official DC FEMS Integrated Response Model report.
External reference: For readers who want to review the national and interagency frameworks that inform DC FEMS practice, the official report on the Integrated Response Model published by DC FEMS in collaboration with NAEMT is an essential resource. It outlines training protocols, equipment standardization, and joint exercise requirements that undergird the city’s integrated response approach. https://www.dcfems.gov/programs/integrated-response-model
How Advanced Life Support Drives Outcomes in DC Fire Rescue EMS
Advanced life support protocols in DC Fire Rescue EMS form the backbone of immediate, lifesaving care across the District. Built on national evidence and guided by the American Heart Association and ILCOR recommendations, these protocols shape every critical action taken by firefighters and paramedics. The integrated response model means that ALS capability arrives with the first engine or medic unit. That proximity shortens the time between recognition and advanced intervention, and it changes what is possible for patients in cardiac arrest, stroke, severe trauma, and other life-threatening emergencies.
At the moment a 911 call is dispatched, protocol-driven care begins. Dispatchers use structured questions to prioritize life threats and to provide scripted instructions when callers are with an unresponsive person. Meanwhile, the closest ALS-capable unit mobilizes. When firefighters trained as paramedics arrive, they begin immediate assessment and treatment under standing medical protocols. This integrated approach ensures chest compressions, defibrillation, airway management, and vascular access do not wait for a separate ambulance. That continuity of care reduces the time to first shock and first medication, two determinants of survival in cardiac arrest.
Cardiac arrest protocols emphasize high-quality, uninterrupted chest compressions and early defibrillation. Teams follow a rhythm-driven algorithm. Compressions are prioritized over pauses, and when a shockable rhythm is detected, defibrillation is delivered promptly. Paramedics secure an airway using advanced devices, and they verify placement with waveform CO2 monitoring. Vascular access is established intravenously or intraosseously to allow medication delivery. Epinephrine dosing follows protocol timing, and antiarrhythmics are used for refractory ventricular arrhythmias. When return of spontaneous circulation occurs, post-arrest care focuses on stabilizing oxygenation, ventilation, and blood pressure during transport to an appropriate receiving facility.
For acute coronary syndromes, field protocols guide rapid assessment and early ECG acquisition. Paramedics interpret or transmit electrocardiograms to receiving hospitals to activate cardiac teams when appropriate. Pain control, oxygen titration, and antiplatelet or anticoagulant considerations follow medical directives. Timely transport decisions and alerts to the receiving center help minimize door-to-balloon times when percutaneous coronary intervention is needed. Stroke protocols mirror this emphasis on time. Paramedics use a validated prehospital stroke scale to identify likely large-vessel occlusion. They perform glucose checks and rapid neurologic checks, then choose destination hospitals based on predefined stroke triage rules. Early notification to the stroke center accelerates in-hospital imaging and treatment, including thrombolysis evaluation.
Trauma care in the field adheres to principles of stopping life-threatening hemorrhage, protecting the airway, and rapid transport to designated trauma centers. DC FEMS paramedics apply bleeding control techniques, including direct pressure and, when indicated, tourniquets. They follow protocols limiting prolonged on-scene time when critical injuries demand rapid movement to definitive care. Spinal motion restriction is applied according to updated guidance that balances injury mechanism with neurologic exam. Airway interventions are tailored to the situation, with advanced airway devices available when necessary.
Paramedic training underpins protocol fidelity. DC Fire Rescue invests in rigorous initial and continuing education. Paramedics receive hands-on practice in endotracheal intubation, advanced airway adjuncts, cardiac rhythm interpretation, and medication administration. Simulation exercises replicate complex scenarios and multiunit responses. Training emphasizes the cognitive flow of algorithms and the teamwork required to execute them. In addition, ongoing quality improvement measures ensure protocols evolve with new evidence. Medical direction and clinical oversight audit performance data, review cases, and recommend adjustments to training and clinical practice.
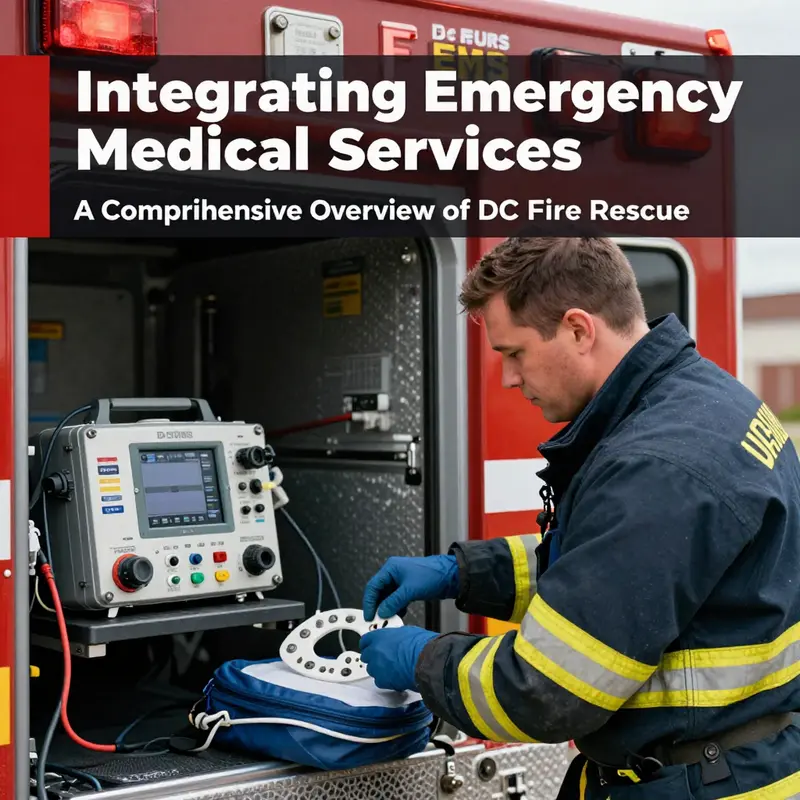
Equipment carried on first-response apparatus reflects the expectation that ALS care will begin immediately. Engines and ambulances stock cardiac monitors with defibrillation capability, advanced airway kits, medications for resuscitation and symptom control, and monitoring tools such as pulse oximetry and capnography. Some units carry specialized capabilities for critically ill patients, including a Mobile Intensive Care Unit. These specialized ambulances bring extended monitoring and advanced interventions to the bedside and during transport when patients require them.
Clinical decision-making in the field is supported by standing orders and protocols that allow paramedics to act quickly without awaiting direct physician approval. When cases fall outside those orders, online medical control provides real-time physician guidance. This hybrid system balances the need for rapid action with physician oversight for complex or unusual situations. Data capture from electronic patient care records feeds back into the system. Trends in response times, rhythm outcomes, medication timing, and neurologic outcomes after stroke are analyzed. These metrics drive targeted training and protocol refinement, improving patient outcomes over time.
Coordination with hospitals and other agencies is built into ALS practice. Prehospital providers communicate with emergency departments to announce critical patients and to clarify destination decisions. For mass-casualty or specialized incidents, DC FEMS coordinates with the Office of Emergency Management and partner agencies. Specialized teams, such as hazardous materials or technical rescue units, operate under clinical and operational protocols that integrate medical care with their unique mission requirements.
Public engagement complements clinical ALS work. Prehospital providers teach CPR and AED use, increasing bystander intervention rates. Community programs emphasize recognition of heart attack and stroke signs, making early 911 activation more likely. These prevention and education efforts extend the reach of ALS protocols by ensuring patients enter the system earlier.
Quality assurance and protocol updates ensure care stays current. Medical directors review evidence and national guideline updates, then translate them into local directives. This process preserves alignment with AHA and ILCOR while adapting recommendations to the District’s operational realities. Continuous training, data review, and targeted feedback loops keep skills sharp. Technology investments in monitoring, data transmission, and feedback systems further support performance improvements; for a discussion on technology and leadership in fire services, see this piece on the impact of technology on fire department leadership.
Taken together, DC Fire Rescue’s ALS protocols combine proven clinical algorithms, thorough training, and real-world operational design. The integrated model places advanced interventions at the earliest moments of an emergency. That approach shortens time to critical treatments, supports better triage and destination choices, and improves the chances of meaningful survival. For official, up-to-date protocol documents and medical directives, consult the District of Columbia Fire and Emergency Medical Services Department’s official website: https://www.dc.gov/service/fire-and-emergency-medical-services
Integrated Speed and Care: How DC Fire Rescue EMS Delivers Life-Saving Care from the Moment the Alarm Calls
From the moment the alarm sounds in Washington, DC, the city’s approach to emergency medicine is a study in unity. The District’s Fire and Emergency Medical Services operates as a single, integrated engine of response, where the line between firefighting and prehospital care is intentionally blurred to save lives. In DC, EMS is not a separate service arriving after a fire engine; it is built into the same response package that appears on the scene. All firefighters are trained as paramedics or EMTs, ensuring that advanced life support care is available the moment responders reach a patient. This on-scene ALS capability turns the critical first minutes of an emergency into a window for definitive care, a difference that matters in cardiac arrests, severe trauma, and strokes where every second counts.
On the street, the apparatus reflect this design: fire engines and ambulances are staffed with medically trained personnel capable of intubation, cardiac monitoring, medication administration, and defibrillation. The first responders can initiate airway management, establish IV lines, administer life-sustaining medications, and monitor rhythm and perfusion while moving toward definitive care. This reduces the time to ALS intervention and creates a continuous level of care from the moment the patient is found through transport. In practice, a patient may receive advanced medical care from the first unit at the scene, with transport teams ready to continue treatment en route to the hospital.
Responding rapidly is not accidental. DC FEMS prioritizes speed as a life-saving variable, supported by a citywide average response time for medical emergencies that is typically under five minutes. Yet speed in a dense urban area depends on more than a siren and a route. It rests on a disciplined, data-informed approach to dispatch, resource placement, and coordination with traffic and road conditions. The system relies on overlap in coverage—fire engines, rescue squads, and EMS units are distributed so that ALS capability is never a secondary option but the primary commitment upon arrival. A cardiac-arrest patient, for instance, may benefit from immediate ALS interventions from the arriving engine, even before a dedicated ambulance can arrive with additional manpower and transport capacity.
DC FEMS maintains specialized units for scenarios that demand more than standard field care. Hazardous Materials teams respond to chemical spills or toxic releases when incidents threaten public safety and environmental health. Technical Rescue units handle high-angle rescues, trapped occupants in confined spaces, and complex vehicle extrications. The Mobile Intensive Care Unit, or MICU, represents the apex of field-level medical capability, a transport platform that carries a physician- or senior-paramedic-led crew with equipment capable of stabilizing and monitoring critically ill or injured patients during transit. The MICU embodies a deliberate balance: rapid access to the patient in danger, followed by high-quality medical support that continues through handoff at the hospital.
Public education and prevention are woven into the operational fabric. DC FEMS conducts CPR and AED training, home safety inspections, and outreach on fire prevention and emergency preparedness. These programs reduce risk and empower residents to act effectively during emergencies, while data-informed prevention efforts help target neighborhoods where risk factors are higher. The integrated model also creates a robust feedback loop: outcomes data feeds improvements in on-scene protocols, post-incident debriefings, and community education programs.
Although DC FEMS is a single agency, its success depends on strong coordination with partners when incidents scale beyond routine calls. The department works closely with the Metropolitan Police Department, the Office of Emergency Management, and other local, state, and federal partners to ensure responders share a common operating picture during large events. This coordination safeguards patient care continuity, aligns medical surge capacity with sheltering and evacuation plans, and maintains coherent public messaging. The integrated structure reduces handoffs, preserves a continuous thread of care from alarm to admission, and supports a unified incident command during disasters.
Beyond daily practice, the latest research in response-time science points to actionable levers for DC FEMS. Machine-learning analyses show that response-time variability is driven by weather, call priority levels, and resource constraints such as ambulance availability and staffing. Gradient Boosting models have demonstrated robustness in predicting a spectrum of scenarios, revealing how weather, traffic, and incident type interact to shape speed. Translating these insights into the field means adaptive resource allocation: pre-positioning units during predicted high-demand periods, adjusting dispatch rules based on weather and real-time traffic information, and crafting routing plans that uphold equity across all call priorities. In other words, speed must be coupled with fairness, ensuring that the most time-critical needs are met quickly across neighborhoods with different density, infrastructure, and access challenges.
Operationalizing these analytics demands careful feature engineering and a culture of evidence-based policy. When DC FEMS applies modeling, scenario testing, and real-time data feeds, it can shift from reactive to proactive deployment. The department’s work aligns with a broader stream of innovation that translates data into front-line practice. This includes initiatives highlighted by the Innovation Museum Transforming Fire Services, which showcases how data-driven design can guide street-level decisions. Innovation Museum Transforming Fire Services.
From a practical standpoint, the daily life of DC’s EMS operation rests on the human factors of teamwork, communication, and situational awareness. Dispatchers triage, prioritize, and coordinate resources to minimize delays, while crews on the street maintain continuous patient assessment and a flexible plan. The MICU’s capabilities complement the core ALS skills on fire engines, not replace them, ensuring rapid stabilization and seamless transfer to hospital care. In this integrated system, handoffs are minimized and information flow is continuous, supporting better outcomes even in the most demanding urban settings. The DC model demonstrates that speed and clinical excellence are not competing priorities but a single, shared objective that guides everything from resource placement to hospital admissions.
Looking ahead, the ongoing challenge is to maintain equity while pushing the boundaries of speed and telematics integration, which will be explored in subsequent chapters. As DC FEMS continues to test predictive models and refine deployment, the next steps will be to translate these insights into policy changes and training evolutions.
External reference: https://www.sciencedirect.com/science/article/pii/S001448352400271X
Specialized Emergency Units in DC Fire Rescue EMS: Precision Teams for a Capital City

In the District of Columbia, an emergency scene rarely begins with a simple one size fits all response. It unfolds as a choreography of specialized units, each trained to address a particular threat while merging into a unified life saving mission. DC FEMS operates as a single integrated system where fire suppression, emergency medical services, hazardous materials response, technical rescue, and public education fuse in practice as well as policy. The capital city complexity – its towering high rises, dense neighborhoods, critical government facilities, and a continuous stream of large gatherings – demands a level of preparedness that goes beyond conventional firefighting. This is where specialized emergency units come to the fore, turning rapid response into rapid, effective action before the patient even reaches a hospital corridor.
The backbone of this approach is an integrated response model in which every firefighter carries the medical training to deliver advanced life support on arrival. This ALS first response capability ensures that time sensitive interventions begin at the threshold of the scene. In a medical emergency seconds matter and those seconds are earned through training, discipline, and the strategic deployment of units designed for specific scenarios. When a call involves potential structural collapse, hazmat exposure, or technical rescue, the same first responders bring not only clinical skill but the right toolset for the job. In DC, every engine and every ambulance is a platform for medicine, and every unit type is a conduit for life saving, with a unified command system guiding operations across the spectrum of emergencies.
Urban Search and Rescue USAR teams stand as a stark reminder of how DC FEMS plans for the worst while protecting the greatest number of people. As a member agency of the National Urban Search and Rescue Response System, DC FEMS USAR teams train to locate, access, and extract victims from collapsed structures after earthquakes, explosions, or other catastrophic events. The work is methodical and technically demanding. Crews move through debris with thermal imaging devices to detect heat signatures, acoustic devices to hear faint sounds, and a repertoire of shoring techniques to stabilize unstable structures. They carry specialized rescue tools that are designed to cut through metal, pry open obstructed pathways, and secure timbers to prevent further collapse. The emphasis is not only on extraction but on minimizing risk to both survivors and rescuers as they navigate unstable environments.
HazMat units represent DC FEMS shield against chemical, biological, radiological, or explosive threats. HazMat teams arrive with a combination of reconnaissance, containment, and mitigation capabilities. They assess scene hazards using instruments and training that anticipate a wide range of contaminants, from household cleaners to industrial toxins. Their protective equipment and operating procedures are designed to reduce exposure for the public and responders alike. The goal is containment at the source, preventing spread to people, water supplies, and surrounding infrastructure, while maintaining the integrity of the incident command structure. In practice HazMat operations require not only technical knowledge but meticulous scene management, because a misstep can convert a local incident into a broader risk that endangers hospitals, schools, and transit hubs.
Technical Rescue Units broaden the reach of DC FEMS beyond the battlefield of fire into the domain of complex rescue. These teams specialize in confined space rescues, rope and high angle operations, swiftwater responses, and intricate extrication scenarios. In a city defined by its vertical architecture and river corridors, the ability to perform delicate rope work on the facade of a high-rise, or to navigate a flooded chamber, is essential. Technical rescue teams train to anticipate equipment failures and environmental hazards, such as shifting loads or low visibility, and they practice coordinating with other units to create a safety cushion around victims. The equipment they rely on—winches, pulley systems, specialized inflatable craft, and a battery of stabilization gear—enables controlled, precise movements when every second counts.
Beyond the specialized teams, Advanced Life Support ambulances form a critical bridge between the scene and hospital care. In DC, ambulances staffed by paramedics provide advanced medical care on the street and during transport. They administer medications, monitor cardiac rhythms, and support airway management, while coordinating with hospital teams to ensure continuity of care. The integration of ALS ambulances with fire units means that the patient receives medical treatment during the earliest moments of response. It also means that transport decisions are informed by on-scene data and the patient evolving condition, rather than waiting for a separate ambulance to establish a line of care after a slower, higher-traffic relay among agencies.
Special Operations Vehicles round out the fleet, providing mobility for large-scale incidents and specialized missions. These are the workhorses that carry heavy equipment, including aerial ladder capabilities for high-rise firefighting and water rescue apparatus for difficult terrain, as well as foam systems and bulk water response units where needed. The diversity of these vehicles aligns with the citys varied geography from crowded downtown blocks to waterfronts and fortress-like government complexes. The presence of such vehicles allows the department to scale operations quickly, shifting from a standard fire suppression mode to a more nuanced, multi-pronged response that can handle both immediate fire control and the meticulous work of rescue and medical stabilization in hazardous environments.
To ensure this constellation of capabilities remains cohesive, DC FEMS relies on a tightly integrated command and control framework. Coordination with the Metropolitan Police Department, the Office of Emergency Management, and other partners is a constant feature of every major incident. In a mass casualty scenario or a multi hazard event, a unified command structure brings together unit chiefs who know the thresholds, capabilities, and limitations of each unit. The aim is not only to deploy the right unit but to synchronize the movement of equipment, personnel, and information so that the window for saving lives remains as wide as possible. Public safety education and prevention activities such as CPR training, home safety inspections, and risk awareness campaigns complement this operational matrix by reducing the number of preventable emergencies and by improving on scene cooperation when calls do occur.
The practical effect of specialized units is most visible in the rapidity of response. DC FEMS prioritizes response times that translate to survival, especially in cardiac arrest, stroke, or major trauma cases. By embedding medical capability within the fire response, the agency shortens the ignition-to-care interval, thereby improving outcomes. The specialized teams also contribute to a city wide culture of preparedness: drills and real world exercises that simulate complex incidents test not only skill but the ability to anticipate, communicate, and adapt. The capacity to switch from a fire focused to a rescue focused or medical focused posture without a long lag is a key advantage in the District, given its multiple high density neighborhoods, federal facilities, and dynamic events calendar.
For readers exploring how this system operates on the ground, the lessons lie in the balance between specialization and integration. The specialized units do not function in isolation; they are designed to reinforce one another. A HazMat call may require safe entry and rescue work, which in turn depends on a technically trained team with the right stabilization gear. A USAR mission may include hazmat considerations if the structural collapse involves contaminants. An ALS ambulance can begin care the moment a firefighter arrives, while the technical rescue crew secures a safe ingress path for both victims and medical providers. The entire enterprise rests on the shared understanding that speed saves lives, but speed must be matched with discipline, professional judgment, and meticulous scene management.
This chapter draws on DC FEMS ongoing commitment to specialized operations and the philosophy that a capital city deserves a force capable of rapid, precise, and safe intervention across a spectrum of threats. The department approach is not static. It evolves with changing hazards, urban development patterns, and the lessons learned from drills and actual incidents alike. Those interested in the strategic mindset behind these capabilities can explore the broader conversation about fire service transformation and innovation in related discussions about modernization and leadership in complex public safety environments. For a sense of the broader innovations shaping such specialized work, see the developments highlighted in Innovation Museum Transforming Fire Services.
In sum, DC FEMS s specialized emergency units are not a luxury but a necessity for a city of its scale and complexity. USAR teams, HazMat units, technical rescue squads, ALS ambulances, and specialized operations vehicles function as an integrated ecosystem. They enable the department to shift rapidly from fire control to rescue and medical stabilization, to manage hazardous environments, and to protect the public and responders alike. This seamless integration under a unified command, supported by interagency coordination, and reinforced by continuous education and prevention work defines how EMS operates within the DC Fire Rescue EMS framework. The result is a system where rapid response and sophisticated capabilities converge, producing outcomes that reflect the unique demands of the District while aligning with national best practices in urban emergency response. For the most current information on vehicle types and configurations, consult the official DC FEMS site.
Beyond the Call: How DC FEMS Builds Safer Neighborhoods Through Community Education and Engagement

Community engagement and public education are not side tasks for DC Fire and Emergency Medical Services (DC FEMS). They are core operational strategies that reduce emergencies, shorten response needs, and save lives before first responders arrive. In Washington, D.C., the agency treats education as a force multiplier: teaching residents to act effectively improves outcomes and helps the unified model of fire and EMS operate more efficiently. This chapter follows how DC FEMS turns outreach into measurable public safety gains, from hands-on training to targeted risk-reduction campaigns.
The foundation of DC FEMS outreach rests on practical, teachable skills. Programs like CPR and AED training give laypeople the confidence to act during cardiac arrest. Knowing how to check breathing, start compressions, and use a defibrillator increases survival odds long before an engine or ambulance arrives. Similarly, the city-wide adoption of the Stop the Bleed curriculum trains civilians to control severe bleeding. Those lessons are simple, actionable, and designed to be taught quickly in workplaces, schools, and community centers. DC FEMS pairs those workshops with clear messaging about when to call 911 and what information to share, which speeds triage and dispatch decisions.
Home fire safety inspections and smoke alarm programs exemplify prevention-focused outreach. DC FEMS personnel or trained volunteers will install smoke alarms, test detectors, and review escape plans with families. Those visits are more than inspections; they are opportunities for risk assessment. Technicians identify hazards such as overloaded circuits, unsafe heating appliances, and inadequate egress for older adults. By addressing these risks directly, the department reduces the likelihood of preventable fires and the related strain on emergency resources.
Schools and youth programs further expand the department’s reach. Fire safety curricula combine interactive demonstrations with age-appropriate drills. Children learn how smoke alarms sound, how to crawl low under smoke, and where to meet outside a home. Those early lessons shape behavior for years. DC FEMS also partners with schools to run emergency preparedness exercises, helping administrators and teachers plan for evacuations and sheltering. These drills reveal gaps in communication and logistics before a real incident, improving readiness across institutions.
DC FEMS recognizes that equitable outreach requires targeted strategies. The city comprises neighborhoods with different vulnerabilities: high-rise buildings, dense apartment clusters, single-family homes, and communities with limited English proficiency. Outreach prioritizes neighborhoods based on data. Dispatch patterns, historical incident maps, and demographic analysis inform where to focus inspections, trainings, and resource placement. Programs for seniors, for example, address mobility constraints and the increased risk of smoke inhalation. Language access services and culturally tailored materials ensure non-English-speaking residents receive clear instructions.
Partnerships are essential. DC FEMS collaborates with the Office of Emergency Management, local nonprofits, community groups, and schools. Such partnerships make outreach scalable and sustainable. Community organizations often provide trusted access to residents. DC FEMS trains community leaders and volunteers to become multipliers of safety information. This strategy extends the department’s influence into neighborhoods that might be harder to reach through patrol or station events alone.
Public events and station open houses offer two-way engagement. Residents meet firefighters and medics in non-emergency contexts, which deepens trust. Trust matters most when callers must give precise details during chaotic situations. Community members who know their local crew are likelier to follow instructions during emergencies and to volunteer by hosting trainings or placing public-access AEDs. These events also provide data: staff record common questions, recurring misconceptions, and local concerns. That information feeds into more effective, targeted campaigns.
Training goes beyond basic lifesaving skills. DC FEMS offers specialized instruction for apartment managers, building supervisors, and institutional staff. For example, building personnel learn how to manage evacuation for residents with disabilities and how to maintain fire doors and suppression systems. Hospital and clinic liaisons receive updates on patient transfer protocols and MICU coordination. This professional-level outreach reduces friction during multi-agency responses and prevents bottlenecks that can impede time-sensitive care.
Technology and innovation support educational goals. Social media channels and the department website deliver timely guidance during heat waves, severe weather, or large public events. Short how-to videos and infographics demonstrate compression depth, bleeding control, and evacuation routes clearly. DC FEMS also uses community feedback tools, such as surveys after trainings, to refine content and delivery. Data from the field—response times, common call types, and demographic trends—inform which messages receive priority in outreach planning.
Community risk reduction (CRR) is the programmatic term for combining data, inspection, and education into a coherent strategy. CRR translates incident data into prevention tasks. If a cluster of kitchen fires emerges in one neighborhood, targeted workshops on cooking safety follow. If overdoses rise in another area, the department coordinates naloxone training and distribution partnerships. CRR budgets time and personnel to the prevention work that reduces future emergency calls.
Measuring impact keeps outreach accountable. DC FEMS tracks metrics such as the number of smoke alarms installed, attendees trained in CPR and Stop the Bleed, and outcomes from bystander interventions. More sophisticated measures include changes in response times and reductions in specific incident categories. When a community shows improved survival rates after a sustained training push, the department validates its approach and scales similar programs elsewhere.
Equally important is accessibility. DC FEMS provides materials in multiple languages and formats. Trainings are scheduled at varying times to accommodate shift workers. Mobile units bring services to pop-up sites and large public gatherings. For residents with hearing impairments or cognitive disabilities, the department adapts instruction through visual aids and hands-on practice. This inclusive approach recognizes that preparedness cannot be one-size-fits-all.
Sustainability of outreach depends on institutionalizing relationships. DC FEMS cultivates a network of certified community instructors and retained partners who can continue training after initial contact. The department also explores sustainable facility design and community-centered station models that host ongoing events. One example of community-centered design is highlighted in an external article about greener, healthier fire stations, which informs how stations can better serve neighborhoods: The Green Firehouse.
Finally, the public’s role is central. Education empowers residents to reduce hazards, respond confidently, and partner with first responders. Those efforts lessen emergency frequency, improve outcomes, and create a resilient urban fabric. For a complete listing of DC FEMS community programs, including scheduling and resources, visit the department’s community engagement page at https://www.dcfems.gov/community-engagement.
Final thoughts
DC Fire and Emergency Medical Services exemplifies a model of excellence in emergency response management through its integrated operational approach. By combining fire services with emergency medical capabilities, DC FEMS ensures rapid and effective care in critical situations. Their dedication to specialized training, efficient response times, and public engagement not only enhances emergency readiness but also fosters a safer community. Understanding these mechanisms allows residents, educators, and emergency personnel to recognize the invaluable role of DC FEMS in safeguarding lives and promoting health within the District of Columbia.